
Hypertension – Don’t blow your top – get it under control!
Introduction:
The modifiable risk factors for our leading killer include hyperlipidemia, diabetes, smoking, and hypertension. What’s the keyword? MODIFIABLE. That means we can do something about it. This is crucial because it means that all hope is not lost. We can do something about these pathologies to decrease our risk of developing cardiovascular disease. So, let’s start with some definitions. Cardiovascular disease includes ***. Hypertension is systolic blood pressure > 120 and diastolic blood pressure > 80. How can you find out about your blood pressure? Should you go to a pharmacy or the Emergency Department (ED) to measure it? Think about that: you are sitting at your local pharmacy; you have a line of people behind you waiting to measure their blood pressure. Or at the ED, you have alarms blaring and oxygen tanks on the walls; it’s not a relaxing day spa. These are not the right environments to get an accurate blood pressure assessment. So, I recommend getting an inexpensive blood pressure cuff from somewhere like Amazon. Pick two specific times per day for seven days and measure your blood pressure. Sit comfortably with your arms at your side – it matters. 1 Don’t worry about the numbers. Write them down and take them to your doctor. This will give them a good assessment of your average blood pressure; if you are above those numbers listed earlier, you have high blood pressure (hypertension)!
This article will discuss the management of blood pressure through the lens of a recent article that looked at a population of folks who presented to the ED with asymptomatic hypertension. So, if you are a medical professional or simply want to understand how to take control of your health, this article is for you!
Title:
Antihypertensive prescription is associated with improved 30-day outcomes for discharged hypertensive emergency department patients. 2
Population:
26.5 million US ED presentations between 2016-2019. 74% of patients who were diagnosed with asymptomatic hypertension (aHTN) were discharged home.
Intervention:
Commencement on antihypertensive treatment in the ED with a script on discharge.
Comparison:
Diagnosis and treatment rates for the following subgroups:
- 160/100 – 179/109 mmHg (Low aHTN)
- >180/110 mmHg (High aHTN)
Outcome:
Different diagnosis and treatment rates per group:
- Low aHTN
o 3.1% diagnosed
o 2.59% treated in the department
o 5.84% given a prescription
- High aHTN
o 13% diagnosed
o 16.2% treated in the department
o 8.4% given a prescription
30,000ft view:
Around 120 million Americans have hypertension that is poorly controlled. 3 A third of Americans have a deadly risk factor – hypertension – for our leading killer. 47% of coronary heart disease and 54% of strokes are attributable to high blood pressure. 4 Let’s sit with that for a moment. If you aren’t horrified, I’m worried. This is a massive problem because it is something that we can act on to help reduce our patient’s risk. To be clear, here we will talk about primary hypertension. There is a category of elevated blood pressure called secondary hypertension. This entity describes a group of diseases caused by pathology involving the vasculature, hormones, and nervous system and is beyond the scope of this article. So, how do we manage hypertension? Like most chronic diseases, we have lifestyle and medications. Let’s break them down.
Lifestyle:
Weight loss
Diet
Sodium reduction
Potassium supplementation
Increase physical activity
Alcohol reduction or cessation
Medications:
There are several types of drugs one can choose from, each with its own benefits for particular situations.
Calcium channel blockers
Beta Blockers
ACE inhibitors
Angiotensin II receptor inhibitors
I strongly encourage everyone to read the American Heart Association (AHA) guidelines for hypertension management. 5 Do not let the weirdo health influencers tell you doctors don’t give advice for lifestyle interventions. They’ll bleat that doctors are all “pill mills,” this couldn’t be farther from the truth!
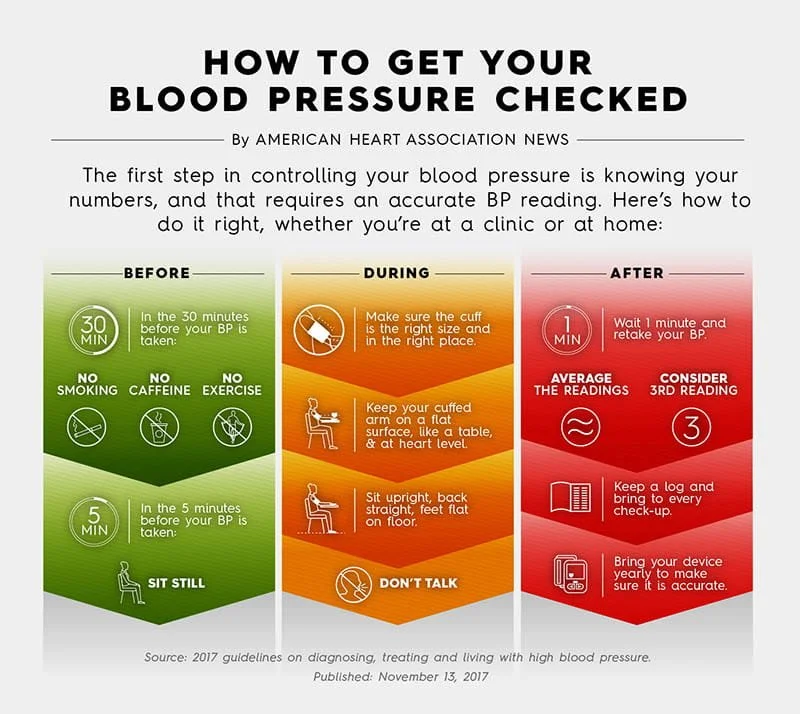
The traffic light system on how to take your blood pressure.
How should this modify your practice:
This is such an important topic. The burden of morbidity associated with poorly controlled hypertension is huge. It is incumbent on physicians to be ready to diagnose and provide support to patients on how to manage their high blood pressure.
Do we need to start antihypertensive agents for these patients? The ACEP clinical guidelines suggest that we do not, and in fact, could cause harm by lowering a patient’s blood pressure too quickly. They do recommend initiating antihypertensive treatment in certain at-risk groups. 6
What is my take? I sit at the end of the spectrum, where we have incredible privileges to help people. In 2024 I am yet to see a person who can establish care with a PCP within a month of the visit to the ED. To say nothing about managing the blood pressure of a patient with aHTN in the ED is doing the patient a disservice. I will spend time with them discussing three things:
1. How to measure their blood pressure, and how to take a log of their blood pressure for when they do see their PCP
2. Lifestyle interventions to reduce blood pressure
a. Weight Loss
b. Diet
c. Exercise
d. Reduced salt and potassium supplementation
e. Alcohol and cigarette cessation
3. Medications – start the conversation with the patient about their values and if those values include commencing medication
So take some action today – diagnose and discuss non-pharmaceutical measures so we can reduce the burden of hypertension in our communities.